Two scientists whose research led to the first approved treatment using the gene-editing tool CRISPR have been awarded a $3 million breakthrough award in the life sciences.
Laureates Dr. Swee Ley Thein of the National Heart, Lung, and Blood Institute (NHLBI) and Dr. Stuart H. Okin of Harvard University shared the award for basic research that led to the development of gene therapies to treat the blood disorders sickle cell disease and beta-thalassemia.
you may like
The Life Sciences Breakthrough Prize has been awarded since 2013 to recognize achievements in the life sciences.
deadly blood disease
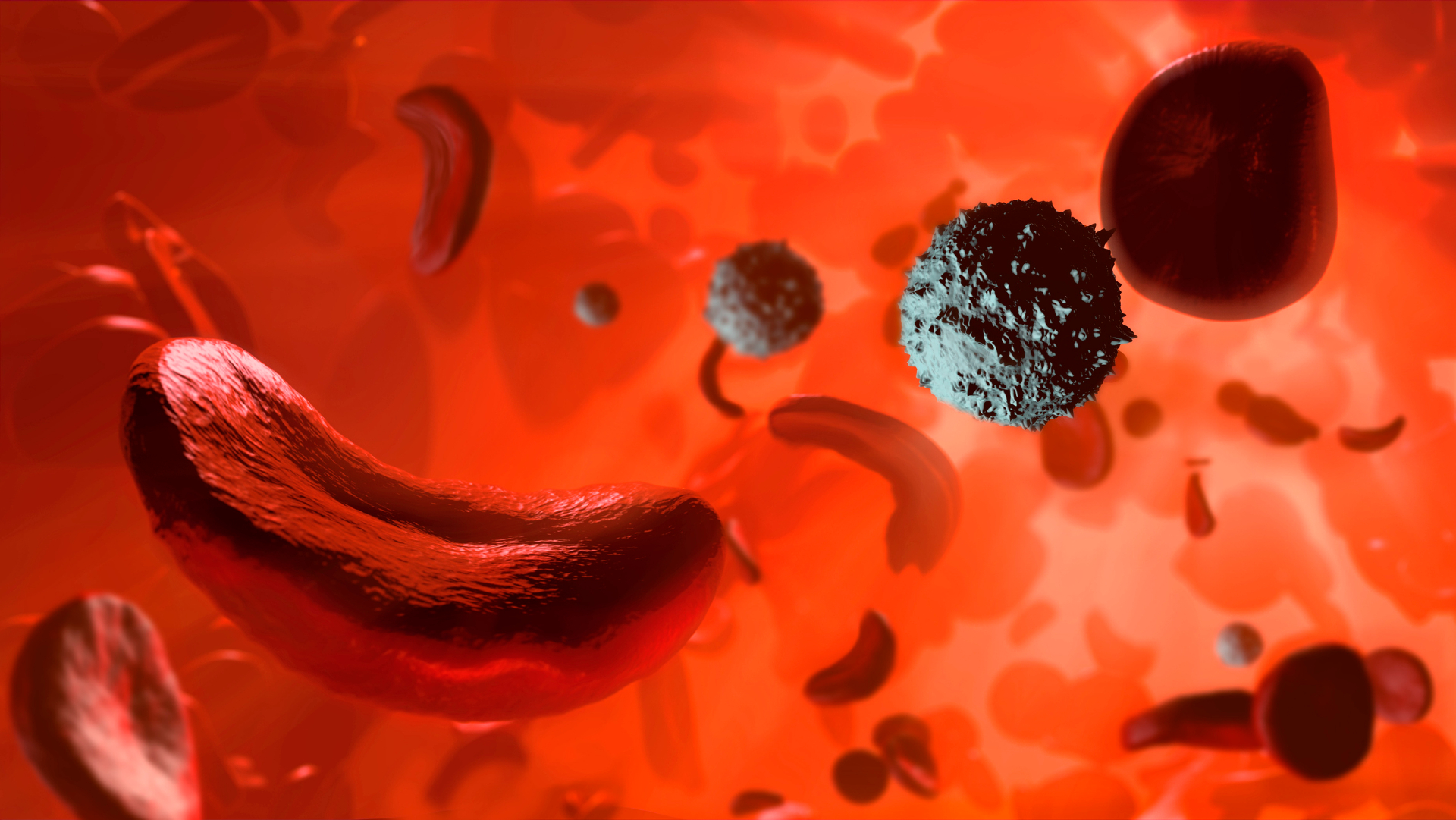
Sickle cell disease affects approximately 7 to 8 million people worldwide, primarily in Africa. In people with this disease, red blood cells take on a characteristic crescent shape because hemoglobin, the molecule that carries oxygen inside cells, forms stiff, long fibrils that deform the cells. These sickle red cells stick together, causing blood clots, and they also rupture and die easily, causing a drop in red blood cell counts.
When red blood cells clog blood vessels, patients often face excruciating pain known as a “crisis.” These blockages can damage organs such as the lungs, liver, and spleen. Lung obstruction can also cause “acute chest syndrome,” which depletes oxygen levels and is the leading cause of death in sickle cell patients.
In beta-thalassemia, the body does not make some hemoglobin molecules or makes less of them. This means that people with severe diseases must receive blood transfusions for the rest of their lives. Kasgebi is approved to treat this severe form of the disease.
Tain, a senior research fellow at NHLBI, began research in the 1980s to understand why some people with these disorders have much milder disease than others.
This question has been around for decades, when New York-based pediatrician Dr. Janet Watson showed that infants who later develop sickle cell disease show no symptoms and their red blood cells do not become sickled.
What to read next
When the children became toddlers, symptoms of the disease appeared.
Follow-up research has shown that humans produce different types of hemoglobin at different stages of development. “Fetal hemoglobin” is produced in the womb, and as the baby grows its production stops and “adult hemoglobin” takes over.

“I started gathering families of people with mild thalassemia to at least figure out the genetics behind it,” Tain told Live Science. “It seemed clear that they had an innate or natural ability to continue producing fetal hemoglobin.”
She analyzed the genes of several families with a history of the disease. Among them were over 200 members, including a family of Indian origin that spanned seven generations and lived on multiple continents.
suppress repressor
Important insights have been gained from studies of monozygotic and dizygotic twin pairs with very high or very low fetal hemoglobin concentrations. This allowed Thein and colleagues to identify genetic mutations that affect fetal hemoglobin production. They focused on a genetic region on chromosome 11 called BCL11A.
Tein’s team discovered that this gene turns off the production of fetal hemoglobin as the baby grows. “It’s a suppressant,” Tain said. However, when people carried certain versions of BCL11A, the repressor was not suppressed and fetal hemoglobin production continued at high levels throughout life.
From there, it wasn’t a dramatic leap to conclude that suppressing the repressor might be a good strategy to treat patients with severe cases of sickle cell disease and beta-thalassemia. Orkin’s research turned out to be extremely important in making that leap forward.
Dr. Orkin, a pediatric hematologist and oncologist at Boston Children’s Hospital, Dana-Farber Cancer Institute, Harvard Medical School, and Howard Hughes Medical Institute, showed how repressors mediate the switch to adult hemoglobin and that gene editing could target this region.
Biotech company Vertex then used the cut-and-paste gene editing tool CRISPR to cut out the repressor region of BCL11A.
This research ultimately led to the development of Kasugevi. Implementing this therapy involves extracting a person’s bone marrow cells, editing the BCL11A repressor using CRISPR, and reinjecting the gene-edited bone marrow cells back into the patient. The edited cells begin making red blood cells that contain high levels of fetal hemoglobin.

It was the first “functional treatment” for sickle cell disease, and it forever changed the lives of the few who received it. However, Thein said the treatment is not available to everyone with the disease and has some drawbacks. The treatment process itself can take up to a year, cost millions of dollars, and require harsh chemotherapy to create space in the bone marrow for the gene-edited stem cells to take root.
“It’s physically very demanding on the patient,” Tain said.
Additionally, sickle cell disease and beta-thalassemia primarily affect populations in Africa, Asia, and the Mediterranean, where the resources and facilities necessary for such treatments may not be available. As a result, scientists working on gene therapy are pivoting to an “in vivo” approach, “actually injecting the gene-editing machine into the patient,” Thein said. This eliminates the need to extract, edit, and reinject bone marrow cells.
Ultimately, Thein said there remains a pressing need for more drugs, such as tablets, injections and IVs, that are cheaper and easier to administer.
Thein researched a drug called Mitavipat. The drug is currently approved to treat the blood diseases pyruvate kinase deficiency and beta-thalassemia, and appears to work by improving the overall metabolic health of red blood cells, Tein said.
She said some patients taking the drug “have been on this treatment with me for six years and it has really made a difference,” but further trials are needed before it can be approved for use in sickle cell patients.
Source link